Amy Stephens
MS, RDN, CSSD, CEDS
Licensed dietitian
specializing in sports nutrition
and eating disorders
MS, RDN, CSSD, CEDS
Licensed dietitian
specializing in sports nutrition
and eating disorders
Use this guide to prevent bone stress injuries and stay healthy.
Bone stress injuries (BSIs) which include bone stress reactions and stress fractures, are often linked to underlying nutrition gaps. The challenge is that the warning signs are subtle and typically appear weeks to months before an actual injury develops. When these early indicators are missed, they can progress into a more serious bone injury that can take an athlete out of training for a while.
Many of these red flags are subtle and easily overlooked, especially in athletes who look strong, healthy, and are performing well. Recognizing and addressing these warning signs early can significantly reduce the risk, and help prevent weeks or even months of missed training and competition.
If you’ve experienced a stress fracture before, reducing risk factors is even more important to prevent another bone injury. The risk of a repeat bone injury is highest within the first year of recovery. Being aware and proactive can help prevent more serious injuries and unnecessary time away from sport.
Here are the most commonly missed nutrition-related risk factors and what to do about them.

Low energy availability (LEA), occurs when your body uses more energy than you consume through food. It can unknowingly happen when workout intensity increases but the food intake stays the same. Some individuals might even see an increase in weight due to an increase in strength but still don’t consume enough food. Food intake needs to be adjusted based on: workout duration, intensity, routine movements (walking) and normal body functions. If there isn’t enough food to cover all of these essential functions, an energy gap develops. There is food energy available for workouts but not other important body functions. During this time, your body prioritizes exercise and movement, even in a low energy state, and downregulates all other non-essential functions which are important for bone health.
In a low energy available state, these functions are downregulated:
Your weight can be stable. Performance can look fine. But your bones and the rest of your body do not have the required energy to recover.
LEA is paramount to the International Olympic Committee’s model of Relative Energy Deficiency in Sport (RED-S)(Mountjoy et al., 2018) and is one of the strongest predictors of bone injury risk (Tenforde et al., 2016). In fact, research shows that bone health can be compromised in as little as five days of underfueling (Papageorgiou et al., 2017).
🚩 Common oversight by athletes: Assuming LEA only exists if weight is dropping. However, increased training intensity, and not just weight loss, drives the injury.
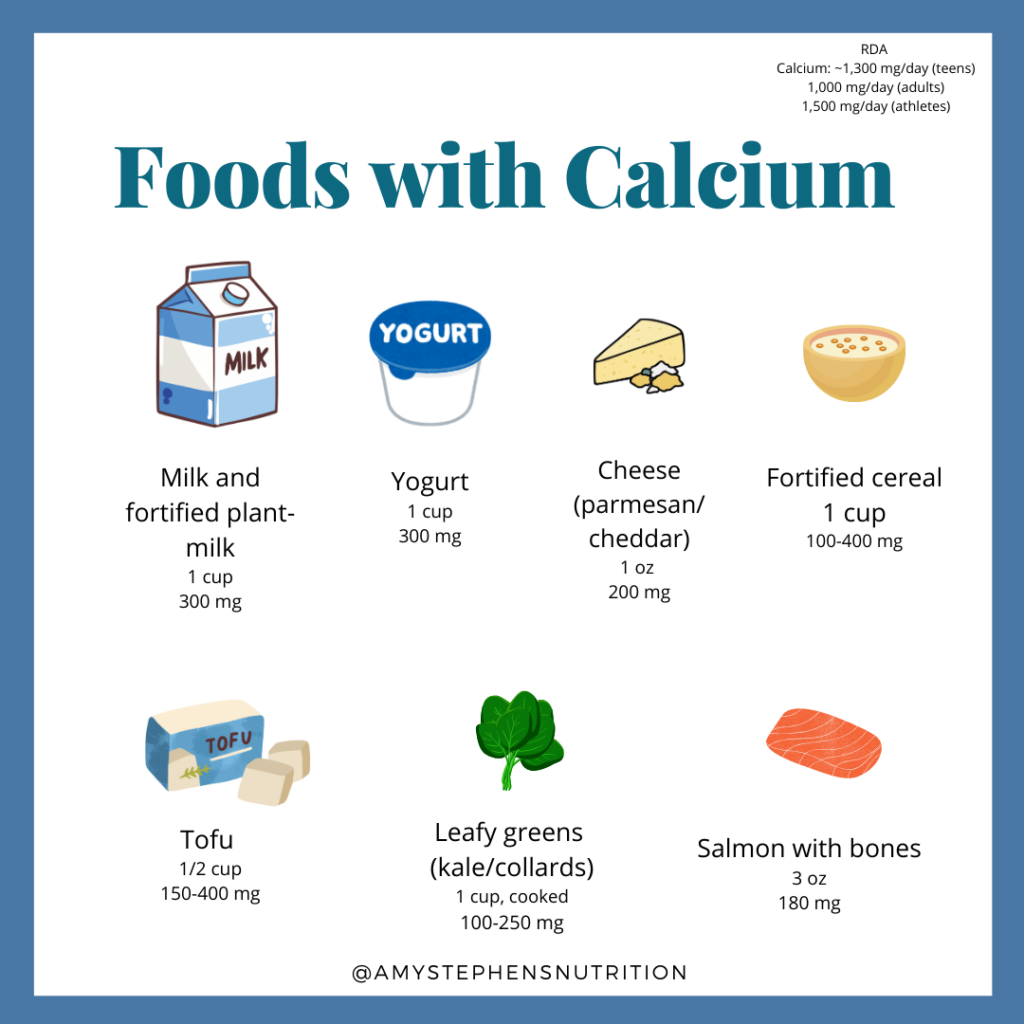
Many athletes assume they’re “covered” because they eat healthy, but calcium intake is often overlooked.
Research in military recruits and runners shows low calcium intake is associated with higher stress fracture rates (Lappe et al., 2008; Nieves et al., 2010). One study found that consuming just one cup of skim milk daily was associated with ~62% lower stress fracture incidence.
🚩 Common miss: Not accounting for daily consistency.
Aim for 3–4 calcium-rich servings daily:
If dairy-free, ensure fortified alternatives are used daily – not occasionally.
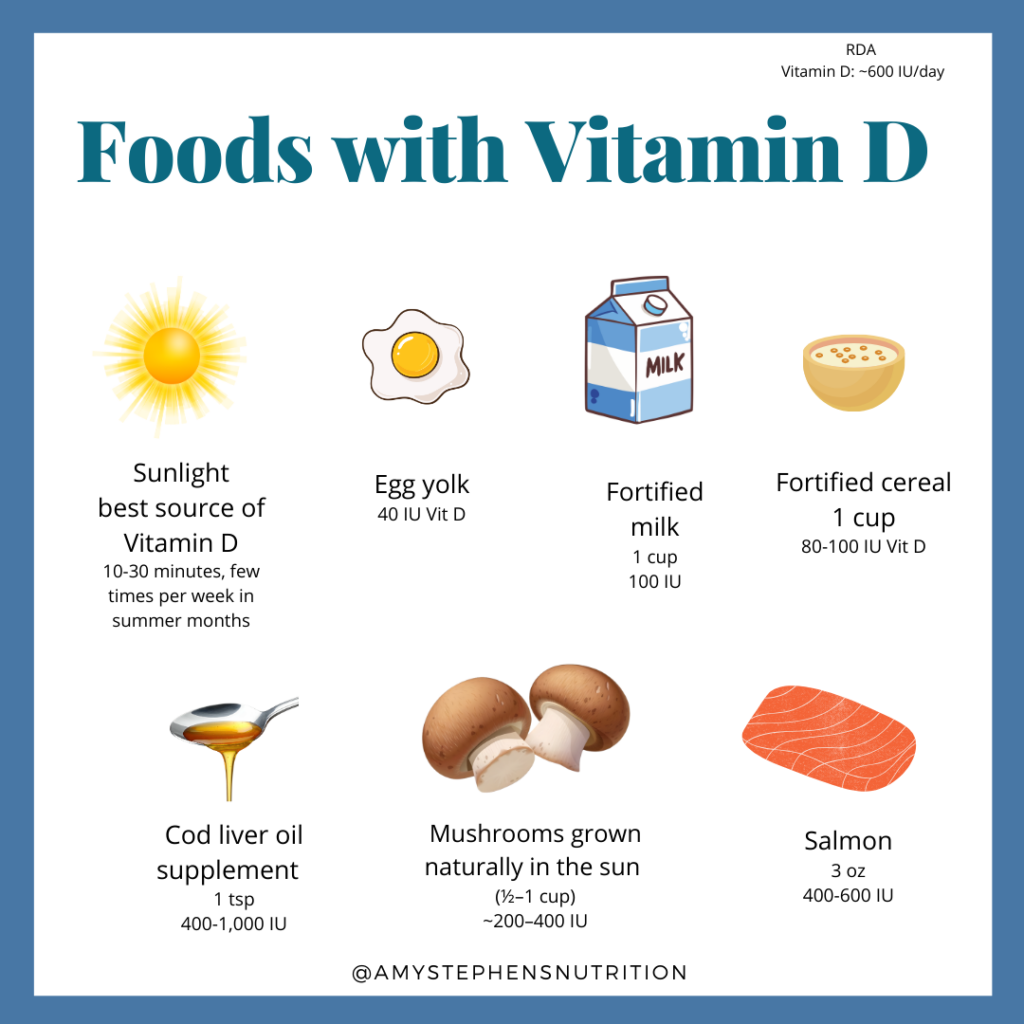
Vitamin D is essential for calcium absorption and bone mineralization. The best source of Vitamin D is from the sun. Athletes can still have low levels even if they train outdoors.
Low Vitamin D levels are associated with significantly higher bone stress injuries (Shimasaki, 2020, Ruohola, 2006). Vitamin D helps the body absorb calcium. Signs of vitamin D deficiency are subtle and include: bone pain, poor mood or low energy.
🚩 Common miss: Waiting for bone pain or other symptoms instead of screening proactively.
Protein isn’t just for muscle, it supports collagen synthesis and bone matrix formation.
Research shows inadequate protein intake negatively affects bone turnover (Heaney & Layman, 2008).
🚩 Common miss: Meeting “minimum” intake but not optimal for training with high quality sources.
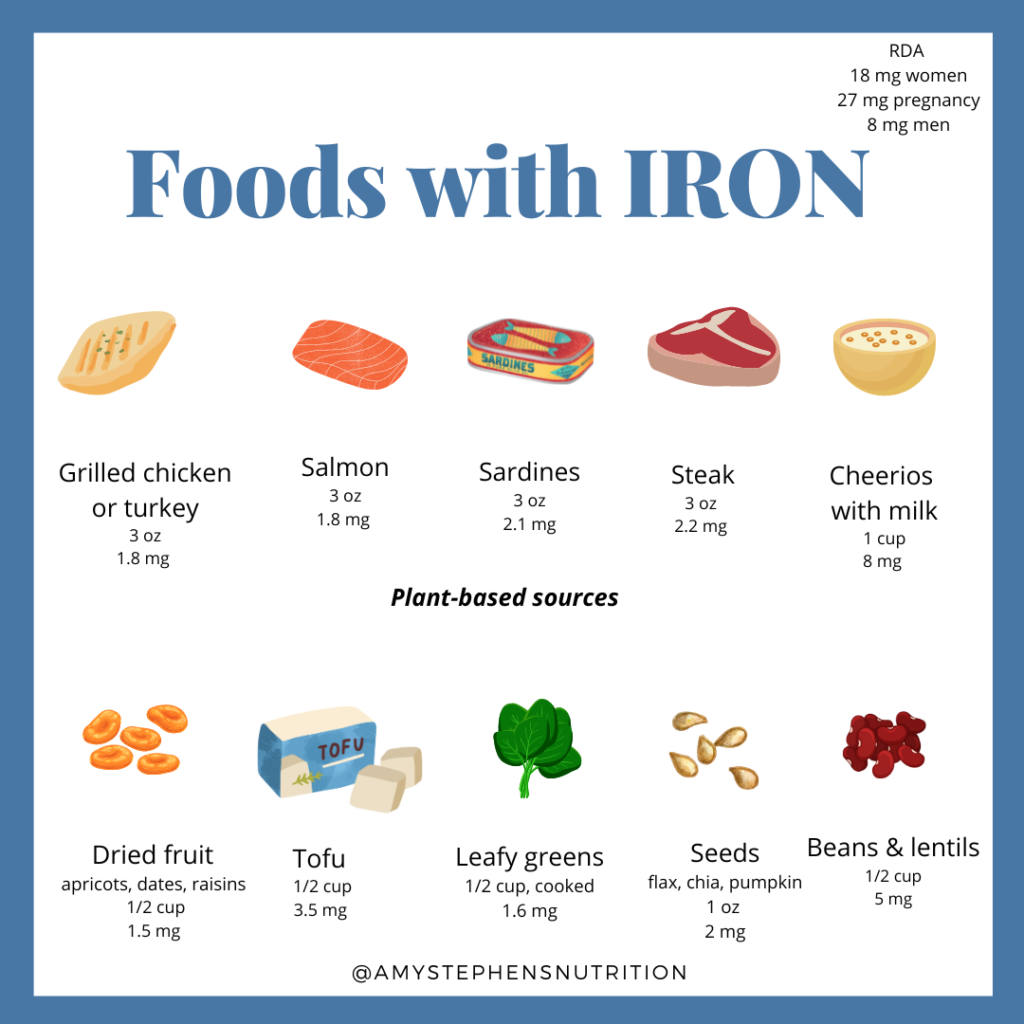
Fatigue is often normalized in sport however iron deficiency is common in athletes with bone stress injuries. Iron deficiency can present as persistent fatigue and low energy, despite adequate fueling.
A 2017 study in Clinical Journal of Sport Medicine found iron deficiency frequently present in female athletes with BSIs (Tenforde, 2017).
Iron deficiency often coexists with low energy availability and RED-S.
🚩 Common miss: Treating iron without addressing underfueling.
An athlete doesn’t need a diagnosed eating disorder to increase bone injury risk. There can be disordered behaviors that prevent an athlete from eating enough food to support exercise.
Research shows disordered eating behaviors independently increase stress fracture risk (Torres-McGehee, 2009).
🚩 Common miss: Waiting until behaviors are severe enough for diagnosis.

“I’ve been fortunate over the course of my 20+ year running career to never suffer a bone injury, even when logging up to 95 miles per week. As I transitioned into coaching and deepened my understanding of the sport, I realized the number one reason for this: I’ve consistently prioritized refueling, especially getting in adequate carbohydrates. The number of high school athletes I see under fueling is staggering, and it almost always connects to the same outcome, injuries, fatigue, and either a plateau or regression in performance. Fueling is one of the simplest aspects of our sport, yet it’s often the most overlooked. If you want to grow as an athlete, you have to feed the athlete.” – Coach Travis Mahoney, TR Performance
Amenorrhea or irregular cycles are not aligned with fitness.
Menstrual dysfunction is strongly associated with increased stress fracture risk and low bone mineral density (Bennell, 1997; Nattiv, 2013).
🚩 Common miss: Referring to missed cycles as “normal for the sport.”
Athletes rarely develop bone injuries from one nutrient deficiency.
They develop them from multiple small fueling gaps that persist over time:
Ask yourself (or your athlete):
“Am I fueling enough to support today’s training and tomorrow’s bone recovery?”
If the answer isn’t a confident yes, it’s worth evaluating.
Early intervention and identification of risks can help athletes prevent injuries that can disrupt a season.
If you’re a runner, athlete, or parent of a young athlete looking for personalized fueling guidance, Amy Stephens offers in-person and virtual nutrition counseling.
Bennell, K. L., Malcolm, S. A., Thomas, S. A., Wark, J. D., & Brukner, P. D. (1997). Risk factors for stress fractures in female athletes. Medicine & Science in Sports & Exercise, 29(7), 949–957. PMID: 9243486
Crunkhorn ML, Etxebarria N, Toohey LA, Charlton P, Watson K, Drew M. The Natural History of Bone Stress Injuries in Athletes: From Inception to Resolution. Sports Med. 2025 Oct;55(10):2415-2428. doi: 10.1007/s40279-025-02280-9. Epub 2025 Jul 28. PMID: 40721688; PMCID: PMC12513886.
Heaney, R. P., & Layman, D. K. (2008). Amount and type of protein influences bone health. Journal of the American College of Nutrition, 27(5 Suppl), 530S–536S. PMID: 18838456
Lappe, J. M., Stegman, M. R., & Recker, R. R. (2008). The impact of lifestyle factors on stress fractures in female Army recruits. Journal of Bone and Mineral Research, 23(5), 741–749. https://doi.org/10.1359/jbmr.080102 PMID:18241246
Mountjoy, M., Sundgot-Borgen, J., Burke, L., Ackerman, K. E., Blauwet, C., Constantini, N., Budgett, R. (2018). IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. British Journal of Sports Medicine, 52(11), 687–697. https://doi.org/10.1136/bjsports-2018-099193 PMID: 29773536
Nattiv, A., Loucks, A. B., Manore, M. M., Sanborn, C. F., Sundgot-Borgen, J., & Warren, M. P. (2013). American College of Sports Medicine position stand: The female athlete triad. Medicine & Science in Sports & Exercise, 45(10), 1867–1882. https://doi.org/10.1249/MSS.0b013e3182a1eaa3 PMID: 23832102
Nieves, J. W., Melsop, K., Curtis, M., Kelsey, J. L., Bachrach, L. K., Greendale, G., Sowers, M. F., & Sainani, K. L. (2010). Nutritional factors that influence change in bone density and stress fracture risk among young female cross-country runners. PM&R, 2(8), 740–750. https://doi.org/10.1016/j.pmrj.2010.04.020 PMID: 20709302
Nieves, J. W., et al. (2010). Calcium and stress fracture risk in female recruits. Calcified Tissue International, 87(4), 329–337. PMID: 20617346
Papageorgiou, M., Elliott-Sale, K. J., Parsons, A., Tang, J. C. Y., Greeves, J. P., Fraser, W. D., & Sale, C. (2017). Effects of reduced energy availability on bone metabolism in women and men. Bone, 105, 191–199. https://doi.org/10.1016/j.bone.2017.08.019 PMID: 28847532
Shimasaki, Y., et al. (2020). Vitamin D status and stress fracture incidence in athletes. Journal of Sports Science & Medicine, 19(1), 59–68. PMID: 32009371
Tenforde, A. S., et al. (2016). Low energy availability in athletes: Causes, consequences, and risk factors. Sports Medicine, 46(1), 1–16. https://doi.org/10.1007/s40279-015-0423-6 PMID: 26553498
Tenforde, A. S., et al. (2017). Association of the female athlete triad risk assessment stratification to the development of bone stress injuries in collegiate athletes. Clinical Journal of Sport Medicine, 27(5), 495–502. PMID: 27359220
Torres-McGehee, T. M., et al. (2009). Eating disorders and the female athlete triad among athletes. Sports Health, 1(5), 379–385. https://doi.org/10.1177/1941738109334218 PMID: 23015865